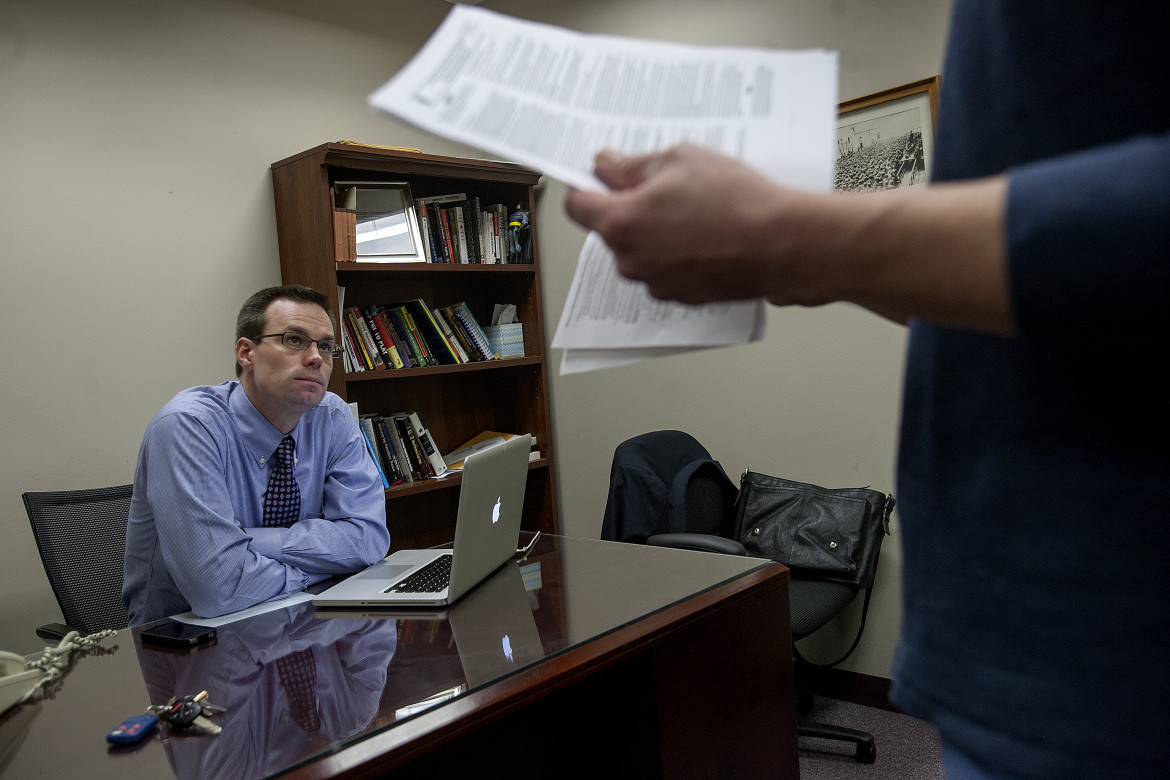
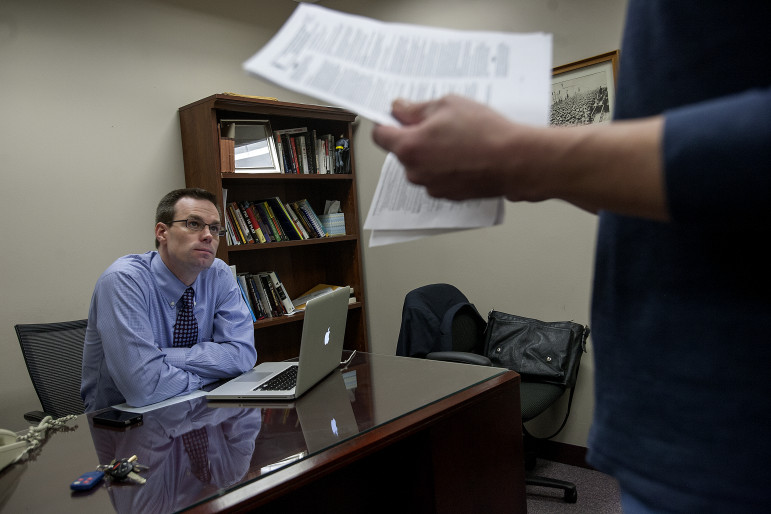
Erik Unger / JJIE
John Maki, executive director of the independent watchdog organization, the John Howard Association of Illinois. The century-old organization is devoted to juvenile and adult prison reform.
Early in 2000, after a groundbreaking study revealed epidemic levels of mental illness among detained youth in Cook County – plus a severe lack of counseling and treatment – the Illinois Department of Human Services launched an ambitious new Mental Health and Juvenile Justice Initiative.
Ever since, the program has been diverting hundreds of emotionally disturbed and behaviorally troubled youth out of the justice system each year and into community-based treatment. Outcomes have been favorable for participating young people and for public safety.
However, for the much larger number of behaviorally troubled youth remaining in the Illinois juvenile justice system – and especially for those committed to state correctional custody – progress has been far slower.
Indeed, the American Civil Liberties Union filed suit in September 2012 alleging that youth housed in state youth corrections facilities still do not receive “minimally adequate” care.
The state settled the lawsuit quickly, agreeing in a December 2012 consent decree to undertake a comprehensive study of its mental health services and institute meaningful reforms. That consent decree, along with other recent changes to minimize confinement of troubled teens and expand the use of research-tested treatment methods, offer renewed hope for mentally ill youth caught up in the juvenile justice system. Yet both advocates and system officials agree that, while the situation is improving, serious challenges remain.

Erik Unger / JJIE
A plaque inside the offices of the John Howard Association of Illinois.
Inside state facilities, “The care is uneven,” says John Maki, executive director of the John Howard Association – a century-old, independent watchdog organization devoted to juvenile and adult prison reform. “They’re juggling a lot of balls: facility consolidation, right-sizing the system, creating a new after-care system.”
Also problematic, says Maki, is the continued reliance on incarceration for some mentally ill youth, and for others with less serious offending histories. “A prison is never the best solution for a kid with serious [mental health] problems,” he says. “Kids always return home. If we can’t deal with kids in the context of their homes and families, we’re never going to fully address it.”
Mental Health and Juvenile Justice Initiative
Initially, the Illinois Mental Health and Juvenile Justice Initiative targeted youth who were locked inside detention centers throughout Illinois and suffered with serious mental illnesses – allowing counties to move these young people into community-based mental health services. The program now operates in every county statewide that houses a youth detention center, though services are no longer limited to youth in detention. The program served 622 youth statewide in 2009, state records show.
An early evaluation, published in the American Psychiatric Association’s journal, Psychiatric Services, found that participating youth improved markedly in terms of both behavior and mental health symptoms. The re-arrest rate for project participants was 42 percent, compared with 72 percent for the overall population of detained youth statewide.
Troubling Treatment for Troubled Youth in State Custody
For mentally ill youth committed to state correctional custody, however, services remained problematic. Until 2006, state youth correction facilities were operated by the Illinois Department of Corrections, and youth were treated similarly to adult prisoners, frequently subjected to solitary confinement. At the state’s facility in Harrisburg, for instance, the John Howard Association found one out of every four youth was locked in seclusion for 23 hours each day in October 2006, spending the remaining hour in a 12-foot by 20-foot cage.
Illinois’ new Department of Juvenile Justice (DJJ) was created to reorient youth corrections facilities toward rehabilitation and treatment, including a beefed up approach to mental health care. But the department made scant progress toward reforming the facilities initially, and criticism reached a crescendo in 2009 following two suicide deaths inside state correctional facilities.
Illustration by Katy McCarthy
Read our full series on Mental Health and the Juvenile Justice System
“Nearly four years following its creation, the Department of Juvenile Justice remains disturbingly far from embracing the treatment mission envisioned by the legislature,” Betsy Clarke, president of the watchdog Juvenile Justice Initiative, told the Illinois House Appropriations Committee in April 2010.
Three months later, department director Kurt Friedenauer, a holdover from the era when youth facilities were part of the adult corrections system, resigned, and veteran child welfare system administrator Arthur Bishop was named to replace him.
Also in 2010, a comprehensive assessment funded by the John D. and Catherine T. MacArthur Foundation found “serious deficiencies” in mental health care for children in state custody, with an inadequate range of programs, a failure to match services to individual needs, and a lack of evidence-based treatment modalities or culturally sensitive services.
The report found that, under Friedenauer, the state had reduced use of solitary confinement and developed a new “core treatment model” that received positive reviews at its initial pilot site, the DJJ youth facility in Chicago. But it faulted the department’s eight facilities—two of which have since been shuttered—for failing to train staff on behavioral health issues and for inadequate aftercare planning and services, especially for youth with mental health and substance abuse issues.
Since 2010, the department has instituted a standardized process to screen youth for mental health issues – a critical failing cited in the MacArthur Foundation report – and upgraded behavioral health training for facility staff.
“We have changed our approach to engaging youth,” Bishop says. “It’s important that when youth are first admitted to us, we can understand the strengths and needs so we can develop discharge plans. We’re no longer waiting until the end, when youth are ready to leave.”
However, more recent analyses have found continuing difficulties. In December 2011, a report by the state’s Juvenile Justice Commission criticized the aftercare services provided to youth released from juvenile facilities, finding that “the Department of Juvenile Justice fails to identify youth needs and does not match identified needs with the services provided to the youth during incarceration.”
Since that report was issued, funding for aftercare programs has increased, and Bishop credits the department with “some success” in adding staff and improving its after-care efforts. However, he acknowledges that progress has been limited due to continued personnel shortages. “The hiring process,” Bishop says, “can be laborious and long. Sometimes that impacts qualified staff, who can’t wait that long. We would definitely note that’s one of the barriers.”
In September 2012, the John Howard Association documented staff shortages at the DJJ facility in Kewanee, Ill., about two hours west of Chicago, that is tasked with treating male youth with the greatest mental health needs.
Only eight of the 17 authorized mental health positions at the facility were filled, the report found. Youth at Kewanee received far less treatment—about 30 minutes per week—than those at other state facilities
“Kewanee is currently unable to fulfill its institutional mission and its constitutional duty to provide the youth in its care with adequate treatment, due to chronically low mental health staff levels. This situation is untenable—legally, ethically and as a matter of public policy,” the report stated.
Since the John Howard report emerged, DJJ has reduced the special treatment units at Kewanee from 90 beds to 54 and moved a portion of its mental health cases to the DJJ facility in St. Charles, Ill., outside of Chicago. The St. Charles facility has added two psychologists and two social workers since February, and it now has two special treatment units with 24 beds apiece.
“In St. Charles, there is a plethora of applicants coming out of the Chicago market,” says Ashley Cross, chief of staff at DJJ.
Staffing problems in Kewanee are nothing new, adds Bishop. “There are no universities in the immediate area” that offer the needed mental health-oriented degree programs, he says. “Part of our discussion is whether or not we can look at another one of our facilities where there is greater availability of professionals to fill critical vacancies. That’s an ongoing review."
Lawsuit and Consent Decree Prompt Hope for Progress
In September 2012, the ACLU filed suit against the DJJ alleging that youth housed in state facilities do not receive “minimally adequate” mental health or education services, are excessively subjected to room confinement for disciplinary reasons (potentially adding to psychological problems), aren’t protected from one another, and are held beyond their release date because adequate community facilities haven’t been identified and placements secured.
The suit noted that two-thirds of confined youth have diagnosed psychiatric and trauma disorders, and it alleged that youth who repeatedly ask for mental health screenings don’t receive them—a failure it cited as a factor in attempted and successful suicides inside state facilities.
The state quickly negotiated a consent decree to settle the case. Under the agreement, signed on December 6, a team of court-appointed experts will investigate all services in the state facilities. For mental health, the appointee is Dr. Louis Kraus, chief of child and adolescent psychology at Rush University Medical Center. The experts will report their findings within six months, and the DJJ will then have 60 days to draft a remedial plan, after which the parties will negotiate a final service enhancement plan, expected later in 2013.
Kraus’ investigation will examine screening and assessment, treatment planning and provision, suicide prevention, prescription and monitoring of medications, substance abuse diagnosis and treatment, juvenile sex offender treatment, and aftercare and discharge planning. These corrective steps must include “sufficient numbers of adequately trained and qualified staff,” including psychiatrists and psychologists, the consent decree notes.
John Maki of John Howard applauds the state’s response to the lawsuit. “I think that takes a lot of courage, and I commend them. A lot of agencies would have fought that,” he says. “This administration is very proactive in looking at what they need to improve upon.”
At Kewanee, “The staffing levels are so abysmally low, they couldn’t possibly begin to provide the care that these kids not only need, but that the state has promised them,” Maki says. “It’s like worrying about your furniture when your house is on fire.”
Not all state facilities have such serious problems related to mental health. In 2012, the John Howard Association lauded the rehabilitative programming and mental health treatment programs at the facility for girls in Warrenville, Ill., and praised the use of evidence-based therapy models at the institution in Chicago, though it noted that continued staffing shortages and limited recreational space still hamper the Chicago facility.
“There needs to be adequate mental health care” for youth in state facilities, says Adam Schwartz, senior staff counsel at the ACLU. “We think the consent decree is a good way to achieve that goal. … We are cautiously optimistic.”
A Need for Expanding Home-Based Care
The ideal solution, Schwartz says, would be to stop placing mentally ill youth into state correctional facilities when they could receive effective mental health services in the community for a fraction of the cost of locking them up. “For the kids who have mental health issues, sending them to somewhere like Kewanee is counter-therapeutic,” he says. “The place looks and feels like a maximum security juvenile prison.”
Especially problematic, experts say, is the state’s widespread use of short-term placements into state facilities. Labeled “court evaluations” – these 30- to 90-day incarceration stays typically do not involve any serious mental health assessment.
“I’ll start cussing now,” Timberlake says with grim humor when asked about these placements. “That shouldn’t exist. It’s an aberration. Sending that child to prison to get an evaluation is a myth, first of all. It’s a terrible way to affect a kid’s life. Incarceration is traumatic, no matter how humane [the facility].”
An August 2012 report by the Illinois Criminal Justice Information Authority found that youth committed for court evaluations typically have less serious offending histories than youth for longer periods. Yet 93 percent of youth released from court evaluation commitments were re-arrested within three to seven years and 59 percent were re-incarcerated in a juvenile or adult corrections facility.
“If the goal of the juvenile justice system is to take a youth who has been adjudicated delinquent and see what the proper placement should be, we think that sending them inside to get the evaluation is a bad idea,” says Schwartz of the ACLU. “There has got to be a way to evaluate them in the community.”
Redeploy Program Shows Promise
In fact, Illinois has initiated a program to divert lower-risk youth away from state correctional facilities and reduce the use of court evaluation commitments. The core of this Redeploy Illinois program is a funding scheme that incentivizes local jurisdictions to keep, treat and supervise nonviolent offenders within their communities, so long as participating sites reduce the numbers of youth committed to state custody by at least 25 percent.
The latest annual report from the Redeploy Illinois Oversight Board found that the eight sites, operating in 28 of the state’s 102 counties, have cut the number of youth committed to DJJ from average of 356 youth per year prior to Redeploy’s launch in 2006 to only 178 commitments per year since.
Also, the annual report found, only 17 percent of youth who successfully complete Redeploy have been rearrested, compared with 73 percent of other juvenile offenders in these same counties, while the subsequent incarceration rate was 14 percent for youth successfully completing Redeploy versus 57 percent for non-participants.
All youth assigned to Redeploy are screened for mental health needs. Based on the screening results, 125 of the 265 youth assigned to Redeploy in 2011 received in-depth mental health assessments and were found to require mental health services, while 165 were assessed for substance abuse and found to require treatment. More than three-fourths of these youth received treatment.
Some sites are using Redeploy funds to provide intensive, evidence-based at-home treatment for participating youth. For instance, St. Clair County’s Redeploy program funds the same Multisystemic Therapy model employed in Cook County. Peoria funds a similar model, Functional Family Therapy, which has also achieved excellent results in clinical evaluation studies.
The average cost of Redeploy programming is less than $10,000 per youth–far less than either an average 8.8-month stay in state custody ($52,000) or a short-term court evaluation ($21,000). The Redeploy oversight board estimates that the program has thus far saved the state $40 million in incarceration costs. But Redeploy does not serve 74 counties including Cook County, home to nearly 40 percent of the state’s youth.
State spending for the Redeploy program -- $2.4 million in 2012 – has declined from $3 million the last couple of years due to tighter state budgets and continues to be dwarfed by state spending for juvenile corrections. Gov. Pat Quinn included a request to double funding for Redeploy in the 2014 budget, but legislative support remains uncertain.
“Redeploy Illinois exists, and there’s no excuse for a community not to join up,” Timberlake says. “It’s the right resource: It spends dollars locally, where people can not only get good services, but also improves the future for that kid.”
The push to reduce the use of incarceration for mentally ill youth and others with less serious offense histories got a boost in 2011, when the Illinois legislature amended the state’s Juvenile Court Act to restrict incarceration for juvenile offenders. Under the new rules, judges may place youth in state custody only as a last resort.
“The push is that judges should …not use the DJJ as a de facto treatment program. Whenever appropriate, youth should be directed to the least restrictive programming setting possible,” Bishop says. “We don’t believe youth that don’t need to be [in DJJ facilities] should be here simply because there may be a lack of services in a particular county,”
Noting that some counties seem to make more than their fair share of court evaluation commitments, Bishops adds. ”We’re trying to drill down and look at why, and make sure judges are complying with legislation that says they should be looking at the least restrictive settings.”
Clarke of the Juvenile Justice Initiative agrees. “Incarceration, in and of itself, is detrimental to mental health. You avoid the trauma of incarceration, which is big, and you’re treating kids in their local communities, you keep them in school, you can work with their families, all of that. It’s far more helpful.”
For JJIE's coverage of mental health treatment for youth in Cook County, click here.
This series is part of an ongoing collaborative with the Center for Public Integrity.